Mallet finger results from flexion or hyperextension forces on the extended distal phalanx, with or without bony avulsion at the distal tendon insertion.
According to the different degrees of distal finger joint avulsion, the classification (picture below) is based on the classification results of Wehbé and Schneider: subtype A accounts for 3%, subtype B accounts for 95.5%, and subtype C accounts for 1.5%.
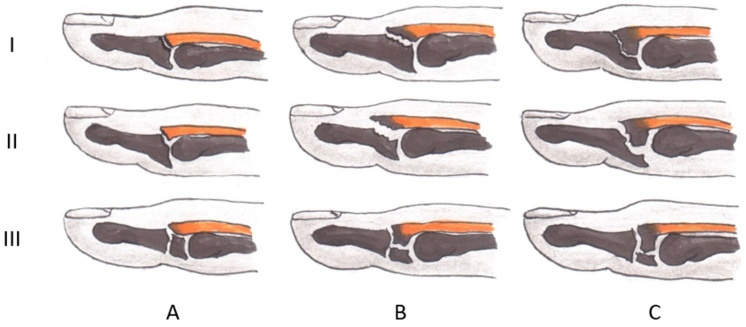
Hammer fingers are classified into different types based on the affected articular surface (subtype A: < 1/3; subtype B: 1/3-2/3; subtype C: > 2/3) and the presence of subluxation (type I1: none Palmar subluxation; type II2: volar subluxation) and growth plate fracture (type III).

The probability of occurrence of pendulous digits in each finger
This article introduces a surgical method of closed fixation using blocking K-wires.
Surgical Needle Insertion Skills
When the distal interphalangeal joint is in the flexion position, a 1.0 mm Kirschner wire is inserted into the distal head of the middle phalanx, and the distal phalanx is slightly hyperextended to attach the bone fragment to the base of the phalanx. The implanted K-wires serve as supports for the bone fragments. Then, drill a second K-wire through the distal interphalangeal joint for fixation.

After 6 weeks, the implant is removed and rehabilitation exercise is performed.
Disclaimer: This article comes from professional journals and books and is edited by Orthopedic Garden. If you have any copyright issues, please contact us.
Post time: Jan-08-2024